Peppermint oil IBS efficacy is scientifically attributed to its primary active compound, L-menthol, which functions as a potent calcium channel blocker in the gastrointestinal smooth muscle. This mechanism significantly reduces colonic spasms, abdominal pain, and bloating. To ensure maximum therapeutic benefit and prevent gastrointestinal reflux, clinical guidelines recommend the use of enteric-coated capsules, which delay release until the oil reaches the small intestine.
The Science: How Peppermint Oil Calms the Gut
To understand the high level of peppermint oil IBS efficacy reported in medical literature, one must look beyond its reputation as a simple flavoring agent. In the context of integrative gastroenterology, which acknowledges traditional healing perspectives like Understanding Te Ao Māori (Māori Worldview) in Rongoā, peppermint oil is a sophisticated pharmacological agent. The primary mechanism of action lies in its high concentration of L-menthol.
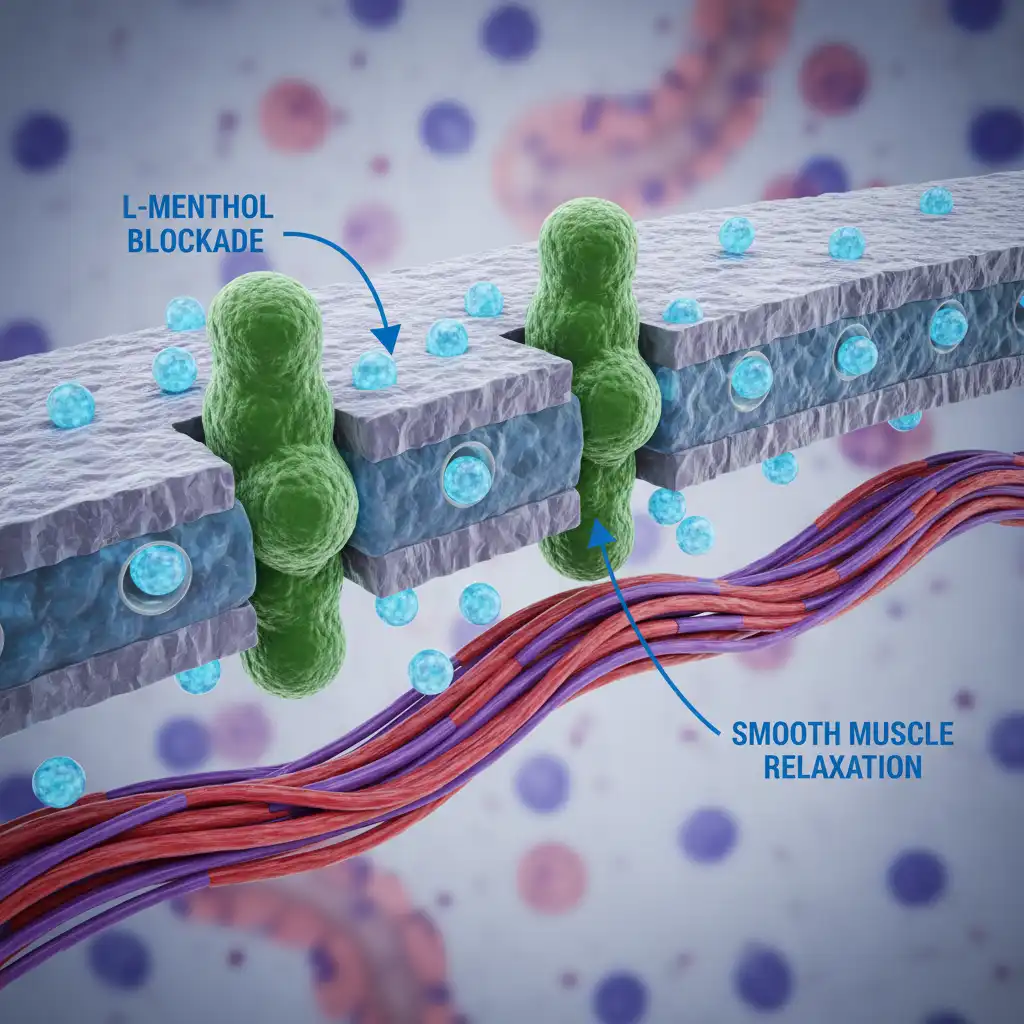
L-menthol acts as a natural calcium channel blocker. Smooth muscle contraction in the gastrointestinal tract relies heavily on the influx of calcium ions into muscle cells. When calcium enters these cells, it triggers the machinery that causes the muscle to contract or spasm. In patients with Irritable Bowel Syndrome (IBS), these contractions are often exaggerated, leading to the hallmark symptoms of cramping, urgency, and visceral pain.
By blocking these calcium channels, peppermint oil effectively prevents the rapid influx of calcium, inducing smooth muscle relaxation. This antispasmodic effect is particularly potent in the colon, where it helps to normalize transit time and reduce the hyper-contractility associated with IBS. Furthermore, research suggests that peppermint oil may possess kappa-opioid receptor agonist activity, which can modulate visceral hypersensitivity—essentially raising the pain threshold in the gut so that normal gas and movement are not perceived as painful.
Anti-inflammatory and Antimicrobial Properties
Beyond its antispasmodic capabilities, peppermint oil exhibits mild anti-inflammatory and antimicrobial properties. Small intestinal bacterial overgrowth (SIBO) is a common comorbidity in IBS patients. The antimicrobial components of peppermint oil can help modulate the gut microbiome, potentially reducing gas production caused by fermentation. This multi-modal approach—targeting motility, sensation, and the microbiome—is why peppermint oil remains a cornerstone of natural IBS management, sharing its esteemed reputation with other botanicals like Tulsi (Holy Basil): The Queen of Herbs.
The Critical Importance of Enteric Coating
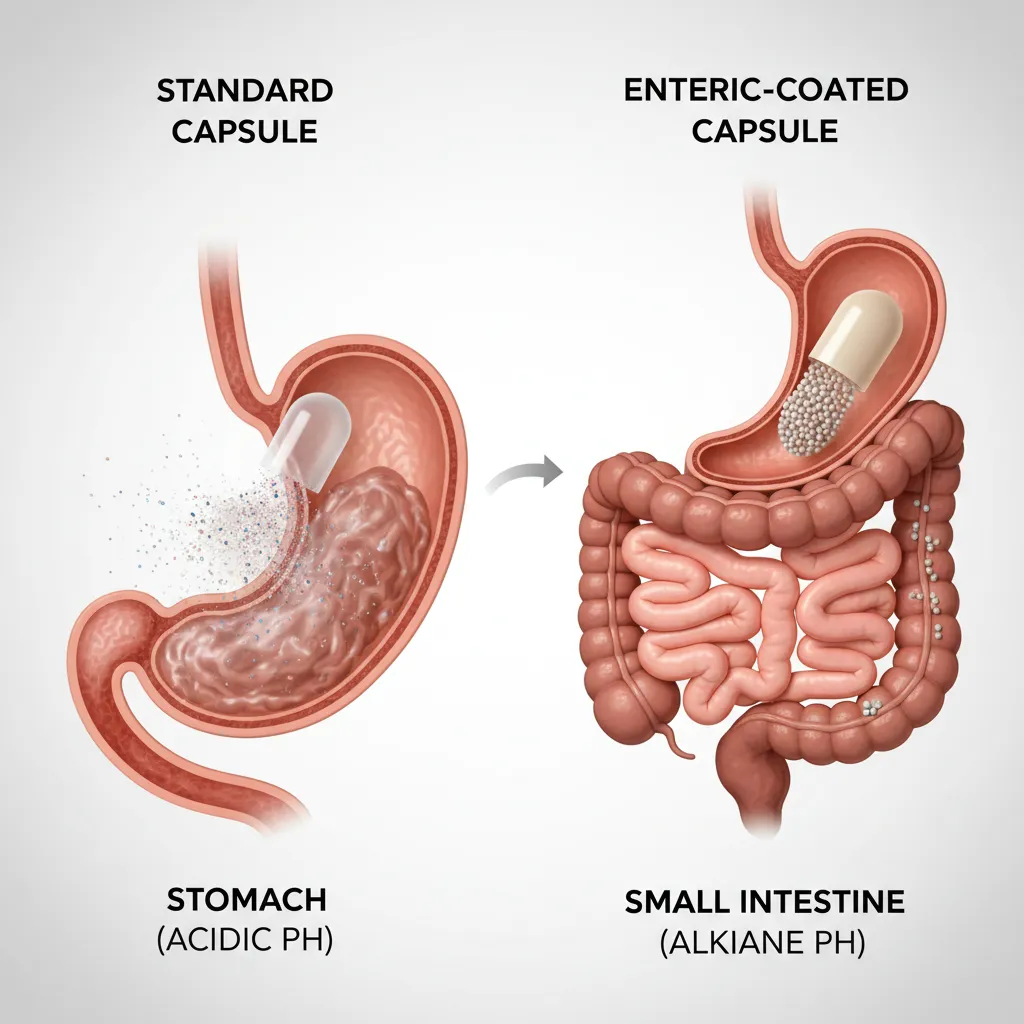
While the efficacy of the oil itself is well-documented, the delivery system is equally important. The term “enteric-coated” refers to a polymer barrier applied to oral medication that prevents its dissolution or disintegration in the gastric environment.
The stomach is highly acidic, with a pH ranging from 1.5 to 3.5. If peppermint oil is released in the stomach, it relaxes the lower esophageal sphincter (LES). The LES is the valve that keeps stomach acid from rising into the esophagus. When this valve relaxes inappropriately, it causes gastroesophageal reflux disease (GERD), manifesting as severe heartburn and indigestion. This is the most common side effect of non-coated peppermint oil preparations and often leads to treatment discontinuation.
Enteric-coated capsules are engineered to withstand stomach acid and only dissolve in the higher pH environment of the small intestine (usually pH 5.5 to 7). This targeted delivery system ensures two critical outcomes:
- Symptom Mitigation: It bypasses the stomach, significantly reducing the risk of heartburn and nausea.
- Targeted Efficacy: It delivers the concentrated L-menthol directly to the duodenum and jejunum, where it can begin its antispasmodic work on the intestines where IBS symptoms originate.
For patients conducting a commercial investigation into which supplement to purchase, verifying the presence of “enteric coating” or “delayed-release” technology is the single most important factor.
ACG Guidelines and Clinical Evidence
The medical community’s acceptance of peppermint oil has shifted from skepticism to endorsement, largely driven by rigorous meta-analyses and clinical guidelines. The American College of Gastroenterology (ACG), the leading authority on digestive health in the United States, has specifically addressed peppermint oil in their guidelines for the management of IBS.
In their comprehensive review, the ACG noted that peppermint oil is superior to placebo in improving global IBS symptoms and abdominal pain. The efficacy data is robust enough that it is often recommended alongside or even before prescription antispasmodics, given its favorable safety profile. A seminal meta-analysis published in the Journal of Clinical Gastroenterology analyzed data from over 800 patients and found that the Number Needed to Treat (NNT) for peppermint oil was approximately 2.5. This means that for every 2.5 patients treated with peppermint oil, one will achieve significant symptom relief—a statistic that rivals many pharmaceutical interventions.
The consensus among integrative health experts is clear: peppermint oil is not merely a “Home remedy” but a clinically validated therapeutic option. However, the guidelines emphasize that efficacy is contingent upon using sustained-release or enteric-coated formulations to ensure the active ingredients reach the distal small bowel and colon.
Dosage Protocols for IBS-D and IBS-C
Determining the correct dosage is vital for balancing efficacy with tolerability. While peppermint oil is generally safe, “more” is not always “better.” Overdosing can lead to anal burning (due to the elimination of menthol) or nausea. The following protocols are derived from successful clinical trials and standard integrative medicine practices.
Standard Therapeutic Dosage
The standard therapeutic dose used in most clinical trials is 0.2 mL to 0.4 mL (approx. 180mg to 225mg) of enteric-coated peppermint oil, taken three times daily.
- Timing: It is crucial to take the capsules 30 to 60 minutes before meals. Taking them with food can alter the pH of the stomach and potentially degrade the enteric coating prematurely, leading to heartburn.
- Duration: Clinical trials often run for 4 to 8 weeks. Many practitioners recommend a 4-week trial period to assess responsiveness.
Protocol for IBS-D (Diarrhea-Predominant)
For patients with IBS-D, the antispasmodic effect is particularly beneficial in slowing down rapid transit time. The relaxation of the smooth muscle reduces the urgency and frequency of bowel movements.
- Start: 1 capsule (approx. 0.2 mL) 30 minutes before breakfast and dinner.
- Titration: If well-tolerated but symptoms persist after 3 days, increase to 3 times daily (before breakfast, lunch, and dinner).
- Maintenance: Continue for 4 weeks, then assess. IBS-D patients often use it on an “as-needed” basis prior to triggering meals once the acute flare has subsided.
Protocol for IBS-C (Constipation-Predominant)
Using antispasmodics in IBS-C requires more nuance. While peppermint oil helps with pain and cramping, excessive relaxation of the gut muscle could theoretically slow transit further. However, because pain is a major component of IBS-C, peppermint oil is still valuable.
- Strategy: Focus on pain management rather than motility.
- Dosage: Lower end of the spectrum (0.2 mL twice daily).
- Combination: It is often best combined with a prokinetic agent (like ginger or prescription motility drugs) or soluble fiber to ensure that while the pain is managed, constipation is not exacerbated.
Safety Profile and Contraindications
Peppermint oil is generally recognized as safe (GRAS) by the FDA, but it is potent. Understanding the side effects and contraindications is essential for safe use.
Common Side Effects:
- Heartburn/Reflux: Even with enteric coating, some patients with severe GERD or hiatal hernias may experience reflux.
- Anal Burning: High doses can result in menthol passing through the digestive tract unabsorbed, causing a sensation of burning during bowel movements.
- Nausea: Usually transient and improved by taking the supplement with a small amount of water (but an empty stomach regarding food).
Contraindications:
- Gallbladder Disease: Peppermint oil can stimulate gallbladder contraction. Patients with gallstones or active cholecystitis should avoid it or consult a physician, as it could trigger a gallbladder attack.
- Severe Hiatal Hernia: The relaxation of the esophageal sphincter can aggravate symptoms in these patients significantly.
- Drug Interactions: While rare, peppermint oil can inhibit certain liver enzymes (CYP3A4), potentially affecting the metabolism of drugs like cyclosporine or calcium channel blockers used for heart conditions.

Peppermint Oil vs. Synthetic Antispasmodics
In the commercial investigation of IBS treatments, patients often weigh natural options against prescriptions. Common synthetic antispasmodics include dicyclomine (Bentyl) and hyoscyamine (Levsin). These drugs work by blocking acetylcholine receptors (anticholinergics).
Side Effect Profile Comparison:
- Synthetics: Anticholinergic side effects are systemic and can be bothersome. They include dry mouth, blurred vision, dizziness, constipation, and urinary retention.
- Peppermint Oil: Side effects are generally localized to the GI tract (heartburn, anal burning). It does not typically cause dry mouth or blurred vision.
For many patients, the localized action of peppermint oil makes it a preferable first-line therapy before attempting systemic anticholinergics. According to research archived by the National Institutes of Health (NIH), the efficacy of peppermint oil is comparable to these prescription agents, often with a higher patient satisfaction rate due to the natural origin and lack of systemic sedation.
People Also Ask
How long does it take for peppermint oil to work for IBS?
Peppermint oil is fast-acting compared to many other IBS treatments. Because it works as a smooth muscle relaxant, many patients experience relief from acute cramping within 1 to 2 hours of ingestion, provided the enteric coating dissolves properly in the small intestine. For global symptom relief (bloating, regularity), consistent use for 1 to 4 weeks is typically required to see maximum benefits.
Can peppermint oil make IBS symptoms worse?
In some cases, yes. If a patient suffers primarily from severe reflux or GERD alongside their IBS, peppermint oil can relax the esophageal sphincter and worsen heartburn. Additionally, for some patients with severe constipation (IBS-C), excessive muscle relaxation might theoretically slow bowel transit, though this is less common than the benefit of pain reduction.
Is peppermint tea as effective as enteric-coated capsules?
No, peppermint tea is generally not as effective for moderate to severe IBS. The concentration of L-menthol in tea is significantly lower than in distilled oil capsules. Furthermore, tea is not enteric-coated; the oil is released in the stomach, which is more likely to cause heartburn and less likely to deliver the antispasmodic compound to the lower intestines where it is needed most.
What is the best time of day to take peppermint oil for IBS?
The optimal time to take peppermint oil is 30 to 60 minutes before a meal, usually breakfast and dinner. Taking it on an empty stomach ensures that the capsule passes through the stomach quickly and reaches the intestines before dissolving. Taking it with food or immediately after a meal increases the risk of the capsule dissolving in the stomach, causing heartburn.
Does peppermint oil help with bloating and gas?
Yes, peppermint oil is highly effective for bloating and gas. By relaxing the smooth muscles of the gut, it allows trapped gas to pass more easily and prevents the painful spasms that trap gas pockets. Its mild antimicrobial properties may also help reduce gas production if bacterial overgrowth is a contributing factor.
Can I take peppermint oil long-term?
Most clinical studies have evaluated peppermint oil for periods of 4 to 12 weeks. While it is generally safe, long-term continuous use is not as well-studied as short-term courses. Many practitioners recommend using it for 4 to 8 weeks to manage a flare-up, and then transitioning to “as-needed” use or cycling off to see if symptoms remain controlled.